


Bite plate (splint) – Myorelaxing
Bite or splints
We usually do bite or myorelaxant splints on patients, who present strong occlusal wears caused by grinding (bruxism) or on clenching patients or with light muscular troubles and on dysfunctional patients.
Realisation
Assemble the models on articulator with the help of the dental face-bow in order to position the upper model in the correct three-dimensional position as the real one of the patient (see the figure).

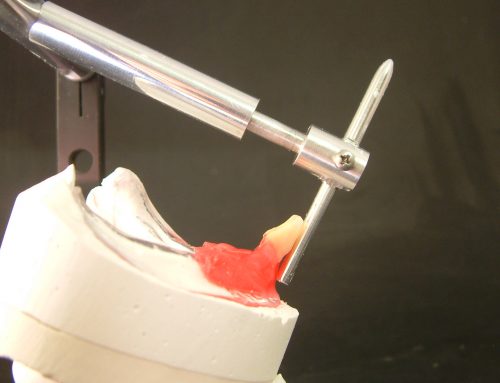
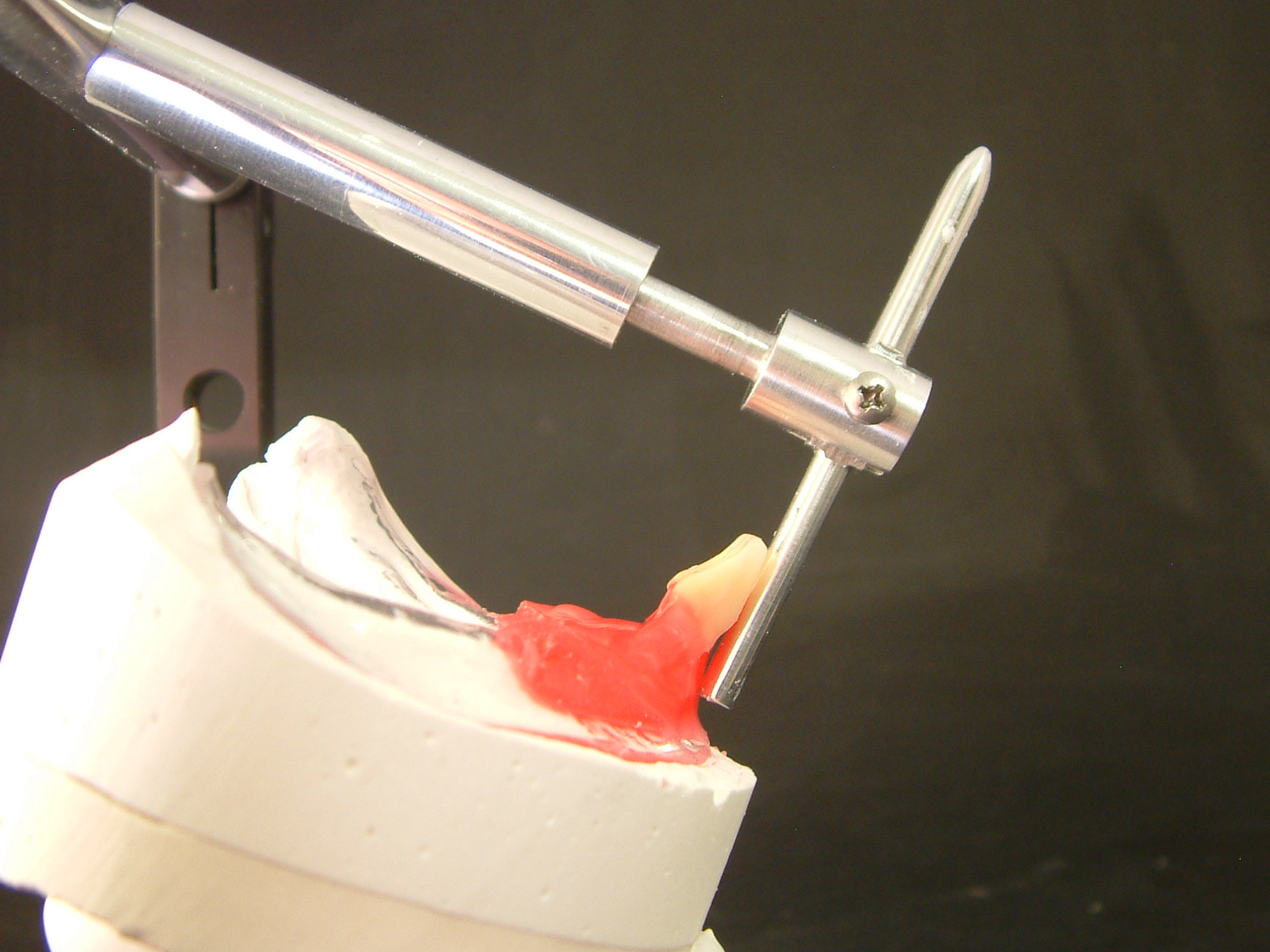
Assemble the lower model on the articulator using the positioning wax (RP) with the articulator incisal rod on ZERO so that, once removed the wax, there is a gap between the upper and the lower model, big enough to realise the bite. This allows to build the bite without raising the vertical dimension on the articulator and to avoid rear rises of the plate once positioned in the patient’s mouth. (See figures).



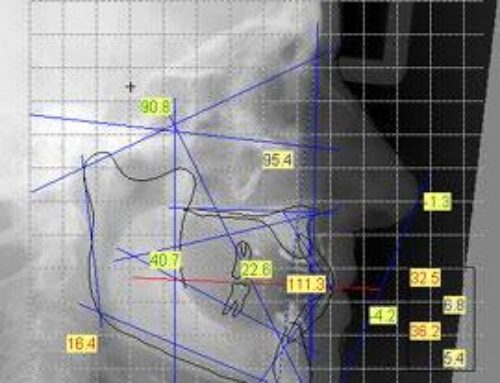
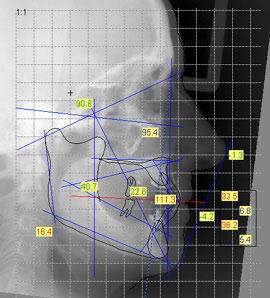
Now it’s necessary to program the articulator with the data, dictated by the axiography or the CPM, with the RP waxes and protrusive technique. (See figures).





Axiography
At this point we can realise the bite; I prefer to press on the lower model a hard thermoplastic disc that is 0,75 mm thick and then cover it with an orthodontic transparent resin, but every technique is good (“salt and pepper” technique or firing in muffle, etc.).
The bite characteristics are very important:
- . Canine guides
- . The front group must touch lightly the antagonist (check with a Shimstock 12µ).
- . The upper palatal cusps must get in touch with each other, while the buccal cusps must not touch to avoid interferences during right and left laterality movements
- . Protrusive check of the upper canine.



{kind=link}
{kind=link}
{kind=link}