


Articular repositioning bite in total removable prosthesis
Foreword
The starting point to build with success two total prosthesis in edentulous patient consists in the fact that he has to be stable at occlusal level and consequently at articular level. What do we mean with occlusal stability? A patient who opens and closes in a fixed position, if possible in RP. We don’t find always this condition, especially in patients with worn out prosthesis and with loss of the vertical dimension. In these cases the patient can have taken a usual advanced posture (third prosthetic class) or he can close in different positions. We need the repositioning plate to give the patient, removable prosthesis bearer, a new position that is more correct in RP, if necessary a new vertical dimension and an occlusal plane of the correct occlusal table. This is possible without altering the old prosthesis or making temporary prosthesis.
To stabilise at articular level an edentulous patient means to reduce quite a lot failures during the planning and building phase of a total prosthesis.
How to realise a repositioning bite
First of all, prepare a cephalometric tracing of the current situation with the old prosthesis in order to determine the right vertical dimension and consequently the correct rise that we have to give the patient through the plate.

Tracciato cefalometrico
Now it’s necessary to assemble the models with the old duplicated prosthesis thanks to a RP wax and to create the rise obtained from the cephalometric values
We can create the rise in the laboratory by compensating for the incisal rod of the articulator, following the directions of the “pin table” provided to us by the cephalometry.
Otherwise plaster with a wax taken to the patient by the clinician with the thickness that we desire to give to the verticalisation bite. In this way we create the rise directly in the mouth so we can plaster with the rod at ZERO. Once removed the wax we have directly created the necessary space for the plate.
The second method reduces a lot the rear pre-contacts once delivered the plate.

Once obtained the necessary gap for the realisation of the plate…

Press with a hard thermoplastic disc (I use a 0,05 mm thick disc) the occlusal surface of the prosthesis we have to modify, which can be both upper and lower, in order to reproduce the existing occlusal table

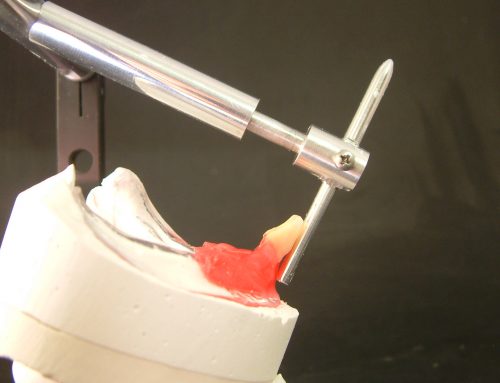
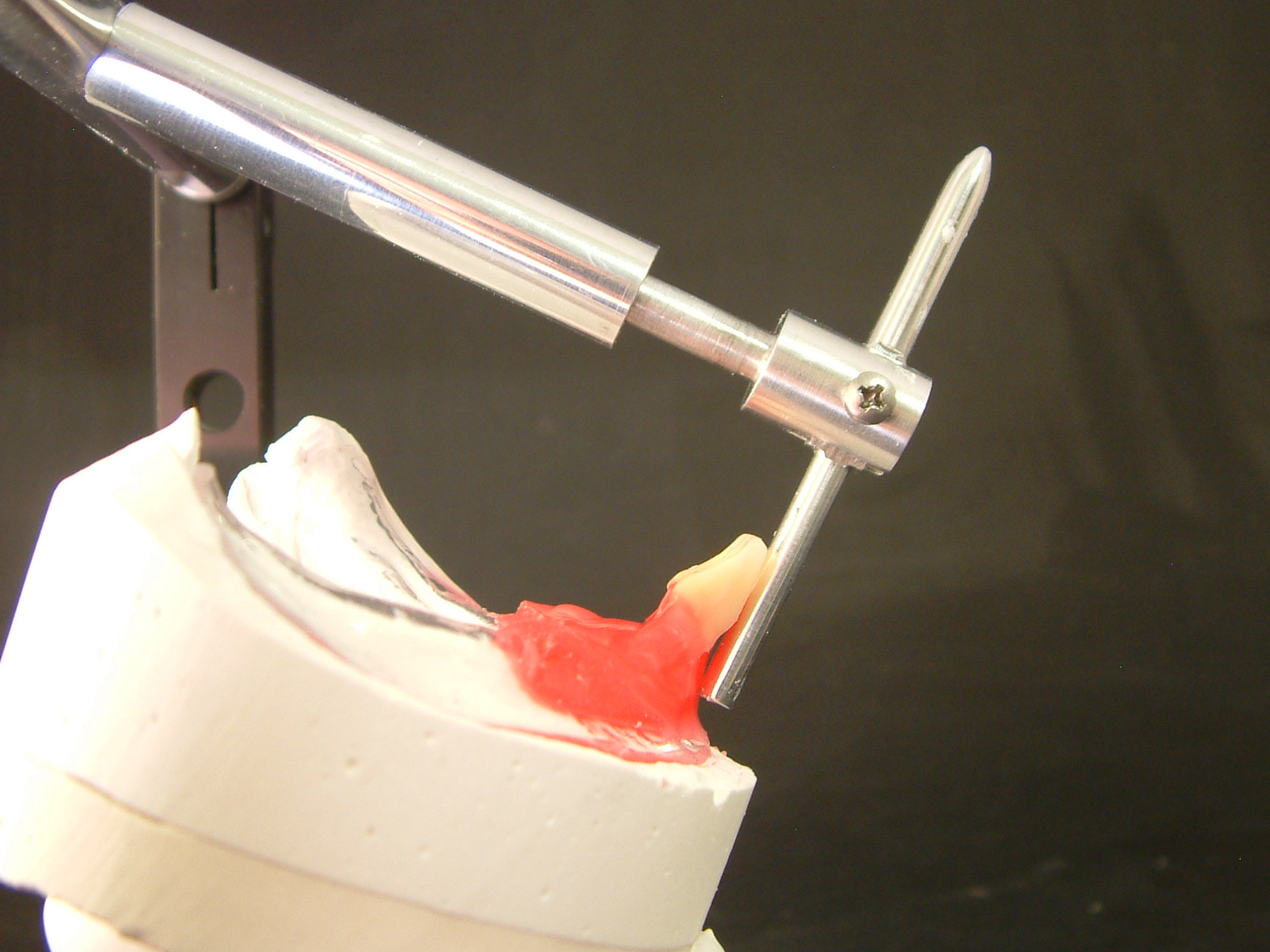
Now find the correct position on articulator.

Inject some resin for temporary prosthesis and polymerize.

At this point nothing remains, that detach the polymerized bite and position it interlocking on the prosthesis.
The clinician will check the new position and the new dimension in several sessions until the patient will find again the occlusal-articular stability. Now we are ready to realise new prosthesis.



BELOW: patient with prosthesis without verticalisation splint and patient with prosthesis with inserted bite, we can observe the immediate aesthetic advantage.




{kind=link}
{kind=link}
{kind=link}
{kind=link}